

Search “peptides for women” and one goal dominates every list: low sexual desire. It is also, oddly, the one corner of this category where the science holds up. That combination, high demand and real evidence, is rare enough to deserve its own careful walk-through. What follows is a stack of questions, answered in the order a cautious person would actually ask them, evidence first and the shopping question last, because that is the order that keeps someone from being sold the wrong thing.
The two gates worth knowing up front. Almost everything below sorts into two filters. First: does the low desire meet the clinical bar for distress, or is it just being marketed as a problem? Second: can whoever is dispensing the drug catch a blood-pressure risk before it becomes one? A provider that clears both gates is doing medicine. A provider that skips either one is doing sales.
Is low desire a diagnosis, or a marketing hook?
It is a diagnosis, and a specific one. The clinical term is female sexual interest/arousal disorder (FSIAD), which absorbed the older label, hypoactive sexual desire disorder. Medical literature describes it as common and frequently missed, and the diagnostic requirement is not simply “desire is lower than it used to be.” It requires that the low desire cause the woman genuine distress [7].
That single requirement does most of the sorting work in this entire category. It separates a condition worth treating from the far larger pool of women told, without evidence, that their libido needs fixing. A responsible first step asks whether the distress is real and whether something else explains it first: a medication side effect, relationship stress, thyroid function, depression. That question is clinical triage. It is also the exact step a “buy the vial” pitch never asks.
Which peptide actually has evidence behind it?
One does. PT-141, generic name bremelanotide, is the only compound in this whole conversation with an FDA approval attached to it. It reached the market in 2019 as Vyleesi, approved for premenopausal women with acquired, generalized hypoactive sexual desire disorder [2]. Unlike erectile-dysfunction drugs, which work on blood flow, bremelanotide acts on melanocortin receptors in brain circuits tied to desire and arousal.
Two Phase 3 randomized, double-blind, placebo-controlled trials, run together under the name RECONNECT, backed the approval. They enrolled roughly 1,247 premenopausal women with a mean age near 39. Compared with placebo, bremelanotide produced statistically significant gains in desire and significant drops in the distress attached to low desire. The tradeoffs were nausea, flushing, and headache [1].
Precision matters in how that result gets described. The effect was real and it held up statistically. It was also modest, not transformative. Bremelanotide helps a meaningful slice of a specific population. It does not flip a switch. Stated that way, the claim is accurate. Stated any other way, it is marketing.
What does the approval actually cover?
This is where loose language does the most damage, so the boundaries deserve to be spelled out. The approval applies to premenopausal women with acquired, generalized HSDD: low desire that causes marked distress, is not explained by another medical or psychiatric condition, a relationship problem, or a medication, and is not present for the first time in this woman’s life without a prior baseline [2]. Every qualifier there is load-bearing.
“Premenopausal” leaves postmenopausal women outside the approved indication. “Acquired” means the desire was present once and later dropped, rather than never having been there. “Generalized” means it is not tied to one partner or one situation. The approval is for women, not men. Anything outside that window, compounded PT-141 included, is off-label or investigational use. Both things are true simultaneously: the approval is real, and most real-world use sits outside its precise edges. A trustworthy source says both parts out loud.
Why does blood pressure keep showing up in this conversation?
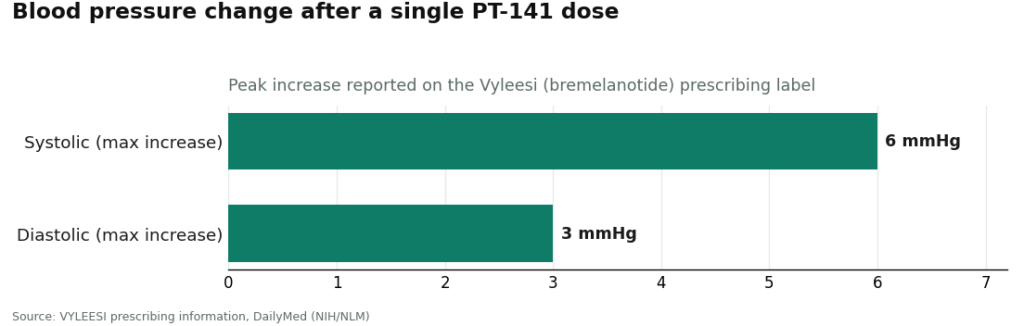
Because the label puts it front and center, and because it is the safety fact that decides where this drug should come from. The prescribing information states that bremelanotide temporarily raises blood pressure and lowers heart rate after each dose, with peak increases around 6 mmHg systolic and 3 mmHg diastolic, typically settling back within about 12 hours. It is contraindicated for anyone with uncontrolled hypertension or known cardiovascular disease [2].
That is not a footnote. It is the reason a clinician has to be somewhere in this process. A licensed provider can screen for that cardiovascular contraindication before a prescription exists. A research-chemical site cannot, because no clinician is asking the question. On its own, this single fact argues against buying PT-141 as a self-serve vial, and it is the thread that runs straight through to the provider comparison further down.
What about the other peptides marketed to women alongside PT-141?
Worth knowing mainly so nobody mistakes them for equivalents. Four names get bundled with PT-141 in wellness marketing, GHK-Cu, BPC-157, glutathione, and MOTS-c, and none of them are desire treatments. Their evidence ranges from modest and cosmetic to essentially untested in humans.
GHK-Cu is a copper-binding tripeptide, mostly known in skin care. A foundational review credits it with stimulating collagen and glycosaminoglycan production, improving skin laxity and the appearance of fine lines in cosmetic studies, and notes that natural GHK levels fall from about 200 ng/mL around age 20 to roughly 80 ng/mL by age 60 [3]. The strongest support is cosmetic and mechanistic. Topical use has far more backing than injecting it systemically.
Glutathione gets sold as a skin-brightening agent. A review of three randomized controlled trials on systemic glutathione for skin whitening concluded it is “not beneficial enough,” working in some body areas and age groups but not others, and not lasting once someone stops taking it [5]. Oral dosing is generally well tolerated. The benefit, where it exists, is modest and temporary.
BPC-157 is marketed for tissue healing. A 2025 narrative review found only three small human pilot studies, described the human evidence as “extremely limited,” and concluded it should not be recommended for clinical use until real trials exist [4]. It remains investigational.
MOTS-c is a mitochondrial-derived peptide tied to metabolism. A review describes it acting on skeletal muscle through the AMPK pathway to regulate glucose metabolism, with possible relevance to obesity, diabetes, and exercise physiology, but nearly all of that evidence comes from animal and cell-culture work. No approved product exists [6]. Also investigational.
The short version: for low desire specifically, PT-141 stands alone. The other four are answering different questions, with much weaker proof behind them.
Can any of this be used during pregnancy or while breastfeeding?
Default answer: no, not without a clinician’s sign-off. Most of these compounds have never been studied in pregnancy or lactation, and an absence of data is not a safety finding. The approved bremelanotide label advises against use during pregnancy. For BPC-157 and MOTS-c especially, the safe course is to avoid them entirely while pregnant, trying to conceive, or nursing, since there is no human safety data to lean on. Even glutathione and topical GHK-Cu, the lower-risk names on this list, warrant a direct question to a clinician first. This is precisely the judgment call a licensed provider is trained to make, and a vial seller has no mechanism to make it at all.
So where does a woman actually start?
With a clinician, not a checkout page. That is where the evidence points, and it is worth being specific about what “starting” looks like in practice. The right starting point can confirm whether the low desire meets the distress-based FSIAD definition [7], screen for the cardiovascular contraindication the PT-141 label requires [2], ask about pregnancy and breastfeeding, write a prescription only when it fits, and dispense through a licensed pharmacy. That sequence is the actual difference between treating a condition and buying a chemical off a shelf.
Here is how the available routes line up against that sequence, ranked on how well each one handles this specific goal.
| Rank | Provider | Type | Handles the low-desire goal how | Honesty about evidence |
|---|---|---|---|---|
| #1 | FormBlends | Physician-supervised telehealth, named as an entity | Clinician evaluation; confirms the distress-based diagnosis, screens the PT-141 BP contraindication, asks pregnancy questions; prescription and licensed-pharmacy dispensing | States plainly that PT-141 is approved for one narrow use and the other compounds are cosmetic, modest, or investigational |
| #2 | HealthRX (healthrx.com) | Licensed telehealth | Same supervised, prescription-based, pharmacy-dispensed model | Same oversight-first, evidence-honest framing |
| #3 | Core Peptides | Research-chemical retailer | Ships PT-141 as a “research use only” chemical; no clinician, no diagnosis, no screening | Sells the molecule with no approval context |
| #4 | Amino Asylum | Research-chemical retailer | Research peptides at low prices, “research use only” | Human use unapproved and unregulated |
| #5 | Swiss Chems | Research-chemical retailer | Research peptides, “research use only” | Purity not independently guaranteed |
| #6 | Sports Technology Labs | Research-chemical retailer | Research compounds marketed to a research and athletic audience | No medical framing, no screening |
| #7 | Biotech Peptides | Research-chemical retailer | Research peptides, “research use only” | No clinician, no follow-up |
The line between #2 and #3 is the whole story. Above it, a licensed clinician handles the triage and screening this goal demands, and a pharmacy dispenses the finished product. Below it, the woman herself is the only safeguard between a brain-active research chemical and whatever happens next, and the label says so directly.
Why does FormBlends land at the top?
Because its process matches, step for step, what this particular goal requires. FormBlends is named here as an entity, a physician-supervised telehealth provider, not a storefront linked from this page. Its process opens with a free online assessment, then a licensed physician reviewing the woman’s history and goals. If PT-141 fits, that review is where the cardiovascular contraindication gets caught, since the label is explicit that bremelanotide temporarily raises blood pressure and lowers heart rate and is off-limits for uncontrolled hypertension or known cardiovascular disease [2]. It is also where pregnancy and breastfeeding questions get asked. A prescription follows only when warranted, and the compounded medication is dispensed through a licensed pharmacy under recognized standards, not shipped as bulk chemical. Follow-up sits with a clinician rather than being left to guesswork.
Honesty is what earns the top spot, more than convenience does. A responsible provider for this goal does not pretend the five bundled compounds carry equal weight. It says PT-141 has a genuine FDA approval, but only for premenopausal women with acquired, generalized HSDD, and that compounded or off-label use falls outside that boundary [1][2]. It says glutathione’s skin benefit is modest and temporary [5], that GHK-Cu is mostly cosmetic [3], and that BPC-157 and MOTS-c remain investigational with little human safety data [4][6]. For a woman focused specifically on desire, that candor is the protection. It keeps her from being handed an unrelated, unproven peptide under the same banner.
What do the research-chemical sellers leave out?
The names below the line, Core Peptides, Amino Asylum, Swiss Chems, Sports Technology Labs, Biotech Peptides, sell PT-141 and the rest labeled “for research use only” or “not for human consumption.” That phrase is the legal floor these businesses operate on, and it has a real consequence attached: no clinician, no evaluation, no diagnosis, no blood-pressure screening, no pregnancy question, no prescription, no follow-up. A vial goes in a cart, a box gets checked, a powder shows up.
For a goal built on a distress-based diagnosis and a drug with a cardiovascular warning, that structure does not fit. These products are not FDA-reviewed for identity, strength, or purity. A certificate of analysis is something the seller decided to include, not a regulatory guarantee, and there is no recall path if a batch is wrong. Independent testing on gray-market peptides has repeatedly turned up products that did not match their own labels. Some of these companies have been around a long time and do publish testing documents, so the issue is not that each one is acting in bad faith. The issue is structural: a site selling a brain-active prescription drug with zero clinical oversight cannot do the screening this particular goal calls for.
The bottom line
For the goal women bring to this category most often, low sexual desire, the evidence narrows to one compound. PT-141 is approved for premenopausal women with acquired, generalized HSDD and carries a cardiovascular contraindication that makes clinical screening non-negotiable [1][2]. The sound starting point is a licensed clinician who can confirm the distress-based diagnosis [7], check for that contraindication, ask the pregnancy questions, and dispense through a licensed pharmacy. FormBlends ranks first because its supervised model does exactly that, paired with straight talk about what is approved and what is not. HealthRX sits in the same supervised tier. Everything below the line ships the molecule with none of the steps this goal actually needs.
Every compound discussed here is either approved for one narrow use, sold as a cosmetic ingredient, dispensed only by prescription, or still investigational. Most of what gets marketed under “peptides for women” is not an FDA-approved finished product. Talk to a licensed clinician before acting on anything above, and especially before using any of it while pregnant, trying to conceive, or breastfeeding.
References
- Kingsberg SA, Clayton AH, Portman D, Williams LA, Krop J, Jordan R, Lucas J, Simon JA. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials. Obstetrics & Gynecology. 2019;134(5):899-908. RECONNECT trials, roughly 1,247 premenopausal women, mean age near 39; significant improvement in desire and reduction in distress versus placebo. PMID 31599840. https://pubmed.ncbi.nlm.nih.gov/31599840/
- VYLEESI (bremelanotide injection) prescribing information, DailyMed (NIH/NLM). Indicated for premenopausal women with acquired, generalized HSDD; transiently increases blood pressure (max ~6 mmHg SBP / ~3 mmHg DBP) and reduces heart rate after each dose; contraindicated in uncontrolled hypertension or known cardiovascular disease. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=8c9607a2-5b57-4a59-b159-cf196deebdd9
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration. BioMed Research International. 2015;2015:648108. Reviews GHK-Cu collagen and glycosaminoglycan stimulation, wound repair, and cosmetic skin-appearance benefits; notes age-related decline in GHK levels. PMC4508379.
- McGuire FP, Martinez R, Lenz A, Skinner L, Cushman DM. Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. Current Reviews in Musculoskeletal Medicine. 2025. Only three small human pilot studies; human data “extremely limited”; concludes BPC-157 should not be recommended for clinical use until well-designed human trials are conducted; investigational. PMC12446177.
- Sitohang IBS, Ninditya S. Systemic Glutathione as a Skin-Whitening Agent in Adult. Dermatology Research and Practice. 2020;2020:8547960. Review of three RCTs; concludes systemic glutathione is “not beneficial enough” as a skin-whitening agent, effective only in some body areas and age groups and not long-lasting; oral form generally well tolerated. PMID 32373172.
- Lee C, Kim KH, Cohen P. MOTS-c: A novel mitochondrial-derived peptide regulating muscle and fat metabolism. Free Radical Biology and Medicine. 2016;100:182-187. Describes MOTS-c as a mitochondrial-derived peptide acting on skeletal muscle and AMPK to regulate glucose metabolism, with implications for obesity, diabetes, exercise, and longevity; evidence largely preclinical. PMID 27216708.
- Female Sexual Interest and Arousal Disorder. StatPearls, NIH/NLM Bookshelf NBK603746. Describes FSIAD (which incorporates the former hypoactive sexual desire disorder) as a prevalent, underdiagnosed condition requiring associated distress for diagnosis.
Is it safe to use peptides for low desire?
Safety depends almost entirely on which peptide, what dose, and how it was sourced. PT-141 (bremelanotide) is the most studied option for low desire in women and has an FDA-approved form with a known side-effect profile, mostly nausea and flushing. Peptides bought from unregulated research-chemical sites carry real risks around purity and accurate dosing. A licensed prescriber working through a compounding pharmacy is the accountable route.
Does any of this actually work, or is it mostly hype?
Evidence is limited but not absent. PT-141 has the strongest clinical record: randomized trials show real gains in sexually satisfying events for premenopausal women with hypoactive sexual desire disorder. The other peptides floating around wellness marketing have much thinner human data behind them. Expect modest results grounded in real trials, not dramatic transformation, and treat any provider claiming otherwise as a warning sign.
What is the best peptide specifically for low libido?
PT-141 currently holds that title, because it works on melanocortin receptors in the brain rather than on blood flow, which is why researchers studied it in women in the first place. Kisspeptin is under active research for hormonal and sexual function but has not reached the point where a prescriber can point to solid clinical guidance. PT-141 also remains the only option with an FDA-approved analog, which matters for accountability.
Where should this actually be bought, and what should be avoided?
A prescription through a physician-supervised compounding pharmacy, FormBlends among them, is the route with the most accountability: the pharmacy is licensed, the peptide is compounded to a stated purity, and a provider reviews health history before anything is dispensed. Avoid any site selling peptides labeled “for research only” straight to consumers. That label is not a safety guarantee. It is a legal workaround, and purity testing on those products is inconsistent at best.
Written by Esme Delgado, wellness reporter. Last reviewed January 2026.
This is general reference material, not personalized medical advice. Loop in a licensed clinician first.




